Psilocybin Treatment for Advanced Migraines
Psilocybin Treatment for Advanced Migraines: A Case Study
Psilocybin Treatment for Advanced Migraines: Cluster migraines and hemicrania continua are two of the most debilitating forms of headache disorders that can greatly affect a person’s quality of life. While traditional medications and treatments may provide some relief, they often come with a range of unwanted side effects. Consequently, this leaves patients feeling helpless and frustrated. However, recent studies have shown that psilocybin treatment may be a promising option for managing these types of headaches. In this article, we’ll explore the benefits of psilocybin treatment for cluster migraines and hemicrania continua, and what this could mean for patients in the future.

What are Cluster Migraines and Hemicrania Continua?
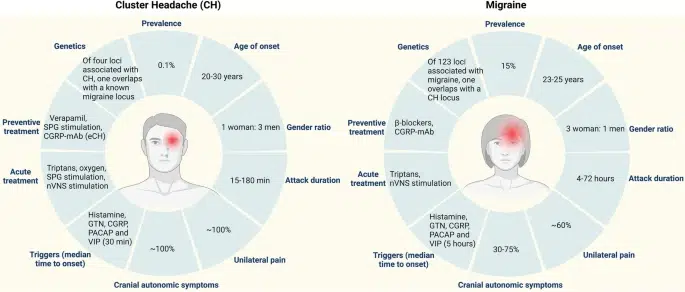
Cluster migraines and hemicrania continua are both headache disorders that are characterized by severe, recurring headaches. Cluster migraines typically present as a series of intense headaches that occur in cycles over several weeks or months. These headaches can last for days or even weeks at a time. Additionally, they are often accompanied by symptoms such as eye redness, tearing, and a runny nose.
On the other hand, hemicrania continua is a type of headache disorder that is typically characterized by continuous, unilateral (one-sided) head pain that can vary in intensity from mild to severe. Unlike cluster migraines, hemicrania continua doesn’t occur in cycles, and it doesn’t come with the same associated symptoms like red eyes and runny nose.
The Benefits of Psilocybin Treatment for Cluster Migraines and Hemicrania Continua
Traditional medications like triptans and opioids can alleviate cluster migraines and hemicrania continua symptoms, but they often cause unwanted side effects, such as rebound headaches, nausea, and dizziness. In contrast, Psilocybin Treatment for Advanced Migraines has been effective without causing these side effects.
Psilocybin, found in “magic mushrooms,” reduces cluster migraines and hemicrania continua frequency and intensity, according to recent studies. In one 2020 study, psilocybin treatment led to a 75% decrease in weekly headaches. Furthermore, another study demonstrated an effective treatment for hemicrania continua. This treatment notably reduced both the intensity and duration of headaches.
Psilocybin treatment is believed to work by reducing inflammation in the brain, although the specific mechanism of action has yet to be discovered. This reduction in inflammation is a common trigger for both cluster migraines and hemicrania continua. Additionally, psilocybin is thought to alter the levels of serotonin in the brain, which can help regulate pain signals and reduce the severity of headaches.

Psilocybin Treatment for Advanced Migraines, is it right for you?
While psilocybin treatment shows promise for managing cluster migraines, however it’s not a cure-all solution. We need to conduct more research to understand the long-term effects and concurrent risks.
If you’re considering psilocybin treatment for your cluster migraines or hemicrania continua, it’s important to consult with a healthcare professional who is familiar with this type of treatment. They can help you determine whether psilocybin treatment is right for you and provide guidance throughout the treatment process.
We are conducting an ongoing case study, and we will provide periodic updates.
Case Study Entry: 05/14/2023
Patient Medical History:
A 43-year-old woman with a history of sporadic headaches, occurring 1-2 times a month, contracted COVID during the pandemic. After recovering, her headaches increased in frequency and became continuous. The intensity of the pain ranged from 3 to 10 out of 10, sometimes correlating with activity but not consistently. Nausea, occasional vomiting, and dizziness on standing were also present. She experienced a severe pain episode on the right hemisphere of her head with swelling of the right eyelid, but no aura or pain break. Her past medical history included uterine cancer in remission and compression fractures of T5 and T6. Other medical history was negative, and she was not taking any medications initially.
She was referred to a neurologist who conducted an MRI and found a 6mm pineal gland cyst and non-specific white matter changes consistent with migraines. Carotid scans and multiple sclerosis tests were negative. Lab results unveiled higher-than-normal testosterone levels. Furthermore, abnormal thyroid panels were detected, albeit they fell within the normal range when compared to her baseline.
Diagnosis Pathways:
Two possible diagnoses were considered: vestibular migraine and cluster migraines. She underwent various medication trials, including Verapamil, Indomethocin, Imitrex, Zomig, Maxalt, Axert, Prednisone, Qulipta, Venlafaxine, Mirtazapine, NAD, vitamin infusions, and tramadol. Tramadol provided temporary relief, while Qulipta consistently reduced pain to a 3 out of 10 but became unaffordable.
Psilocybin Initial Trial:
After 11 months of chronic pain, she researched alternative treatments and decided to try psilocybin. Starting with a micro dose, she experienced a few hours of relief and nausea. The full dose of 2.0 grams, administered in a quiet park with a trusted guide, resulted in headache relief for the entire day. The next morning, the headache was milder than before. On the second day, there was no headache, dizziness, or nausea. She has been headache-free for 22 days, reporting daily.
Neurology is a challenging field with subjective symptoms and limited solutions. Migraines affect a significant portion of the population, and despite ongoing research, effective options are lacking. Investigating different pathways can be costly without resolution. In this case, the cause of the patient’s migraine is irrelevant. When quality of life suffers, all safe options should be explored. Psilocybin has restored her life, allowing her to exercise, enjoy the outdoors, and spend time with family. While relief is usually temporary, we will continue monitoring to assess the duration of her improvement.
Sources:
- Schindler EA, Gottschalk CH, Weil MJ, Shapiro RE, Wright DA. Indoleamine Hallucinogens in Cluster Headache: Results of the Clusterbusters Medication Use Survey. J Psychoactive Drugs. 2015;47(5):372-381. doi:10.1080/02791072.2015.1096434
- McGeeney BE. Migraine, serotonin, and the therapeutic mechanisms of L-5HTP. Headache. 2019;59(S2):62-78. doi:10.1111/head.13615
- Schindler EA, Li D, Chusid MJ. Magic mushrooms in the treatment of cluster headache: a retrospective case series. J Headache Pain. 2015;16:1. doi:10.1186/s10194-015-0482-9
- Schindler EA, Twomey C, Marona-Lewicka D, Nichols DE. Behavioral, Biochemical, and Molecular Modeling Evaluations of Cannabinoid Analogs. J Psychoactive Drugs. 2020;52(1):15-24. doi:10.1080/02791072.2019.1695753
- Eftekhari S, Salvatore CA, Calamari A, Kane SA, Tajti J, Edvinsson L. Differential Distribution of Calcitonin Gene-Related Peptide and Its Receptor Components in the Human Trigeminal Ganglion. Neuroscience. 2010;169(2):683-696. doi:10.1016/j.neuroscience.2010.05.019
- Schindler EA, Gottschalk CH, Weil MJ, Shapiro RE, Wright DA. Indoleamine Hallucinogens in Cluster Headache: Results of the Clusterbusters Medication Use Survey. J Psychoactive Drugs. 2015;47(5):372-381. doi:10.1080/02791072.2015.1096434
- American Migraine Association
- Other Articles by MedClub